
Go inside the international network of women willing to break the law to give people access to termination of pregnancy services.
“Please, please help me. I don’t even sleep anymore.”
“im on my knees now please help now.”
“I dont work im a student confused in a difficult situation dont have a plan.”
Each day, the emails arrive in the inbox of the Dutch charity Women on Web by the hundreds. They come from across the world, in more than a dozen languages. Some are breathless and panicked, others clipped and dispassionate. But stitched together, they often seem to tell a single story.
“the pregnancy is growing so thats why im stressing too much.”
“my parents believe its not worth it that i continue in school if expecting.”
“my mom is going to chase me out of the house if she finds out.”
“abortion is illegal here.”
“Abortion medication is not available in my country.”
“can you help?”
“would you pls help me?
All these notes came from Southern Africa and, across the region, theirs are familiar stories. Abortion is largely illegal in this part of the world (South Africa, Zambia and Mozambique are among the exceptions), driving desperate women wanting to end their pregnancies into the hands of a shadowy network of doctors, herbalists and conmen, who promise – with various degrees of sincerity – pills, plants and procedures that they say can get the job done.
Globally, about 20-million unsafe abortions are carried out each year – nearly all of them in the developing world, according to a paper published in The Lancet medical journal in 2006.
Now, however, more and more women are turning to at-home, do-it-yourself abortion drugs that are mailed thousands of kilometres across continents and to countries where the procedure is illegal. They are breaking the law to get the pills that will, they believe, be far safer than back-alley abortions.
“We are very unapologetic that abortion is a human right that doesn’t depend on borders,” says Leticia Zenevich, helpdesk and outreach co-ordinator for Amsterdam-based Women on Web, which offers advice and, in some cases, the actual pills, to women seeking to terminate their pregnancies in countries where there is no legal avenue to do so.
But these self-induced abortions are deeply controversial, raising tough questions. Does allowing women to perform their own abortions make them more empowered, giving them more control over their own bodies and reproductive health? Or does it simply open them up to new risks, particularly in places where those who perform abortions can be criminally prosecuted?
Misoprostol was never intended to be an abortion pill, let alone revolutionise women’s health across the world. Instead, it was developed for the treatment of peptic ulcers and was widely marketed under the name Cytotec since 1985. The drug carried a warning label: “Poses a serious risk of miscarriage.”
By the late 1980s women in Brazil had cottoned on to the warning. Abortion is illegal in most cases in Brazil, and is now being challenged even in cases of rape. Brazil was the first country where the widespread use of the drug for pregnancy termination was reported, according to a 2012 study published in the journal International Perspectives on Sexual and Reproductive Health. The pills were relatively cheap and didn’t need to be refrigerated, making them ideal for areas where electricity was lacking. Word of the drug soon spread throughout Latin America and beyond.
In recent decades, countries where termination of pregnancy is legal have registered misoprostol for use in medical, or pill-based, abortions. Another abortion pill called mifepristone has also been listed on the World Health Organization’s (WHO) list of essential medicines since 2005. This list, updated by the WHO every two years, is designed to help countries to decide which drugs should be available. Pregnancies can be terminated by medical abortions (using the combination of misoprostol and mifepristone) until the 10th week, the WHO guidelines state.
The WHO recommends that a dose of mifepristone is followed by misoprostol between 36 and 48 hours later, under “close medical supervision”. A 200mg pill of mifepristone blocks the hormone progesterone that is needed for a pregnancy to continue, according to a study published in 2001 in the Journal of the Indian Institute of Science. This causes the lining of the uterus to break down and the embryo detaches from the uterine wall. After one or two days, four misoprostol tablets help to expel the embryo.
Medical abortion, which avoids invasive surgery, is “the most important advance in reproductive health technology since the discovery of oral contraceptives”, argues a 2012 International Perspectives on Sexual and Reproductive Health study. It has been shown to be safe and up to 98% effective for first-trimester termination, according to the study.
In South Africa, as in most other countries where medical abortion is legal, this means the mifepristone pill is taken at a health facility and the misoprostol later, at home.
Early termination of pregnancy using mifepristone and misoprostol has been legal in South Africa since 2001 when medical abortion became available in the private sector. In 2010 the Western Cape became the first province to make medical abortion available in the public health sector to women who were between four and nine weeks pregnant, according to a 2017 study published in the journal of Reproductive Health.
But mifepristone has been registered in fewer than 50 countries, states a study published in 2011 in the British journal BMJ Sexual & Reproductive Health. (By July 2009 it was available in only some African countries: Ethiopia, Ghana, South Africa and Zambia, information published online by Ipas, a global reproductive health and rights charity, reveals.)
Misoprostol, on the other hand, has been licensed as a peptic ulcer drug in more than 90 countries, and is comparatively cheap. Misoprostol alone is widely used to terminate pregnancies when mifepristone is unavailable. The WHO recommends three repeat doses at intervals of at least three hours.

Alice, who prefers not to use her real name, was 20 when she moved to Windhoek four years ago from a tiny windswept Namibian village 800km to the northeast. “I was excited, I was coming to the big city, I thought ‘I can’t wait to see what’s here for me’,” she says. Warm and effervescent, she had little trouble making new friends, or meeting men.
Alice had only been in the city a few weeks when she missed a period. When she confessed her dilemma to a friend, she asked what type of birth control Alice had been on.
“And I said to her, ‘What is birth control?'”
The friend laughed. “You really don’t know?” she asked.
When Alice shook her head no, she told her not to worry.
“I know some guys in a pharmacy,” Alice’s friend said. In Namibia, there are many black market dealers of misoprostol, sold under the brand name Cytotec. Contact information is passed quietly from woman to woman. Some import the drugs from South Africa. Others, like Alice’s friends, buy them illegally from pharmacists.
The next night, her friend handed her a tiny packet of white pills. “She told me to drink one and insert two inside of me,” she says. Within a few hours, “the pain was a 12 on a scale of 1 to 10”.
But still Alice’s friend counselled her not to go to the hospital. Not yet. If she hadn’t had the miscarriage yet, she explained, the doctors might still be able to stop it. So, they waited. As the sun began to rise, with Alice delirious with pain, her friend called a taxi.
“When I told them at the hospital I had a miscarriage, the nurses looked at me like they knew,” she says. But what choice did I have? she wanted to say.
Instead, she was silent.
“When you do a thing like that, it never leaves you,” she says. “You can move on from something like that but you can’t forget.”
Are you in South Africa and need to terminate a pregnancy safely and legally? Find a designated public abortion clinic via Bhekisisa’s new #SizaMap and call the clinic nearest you for more information.
As in many parts of the world, information on how to poison a pregnancy out of your body is passed among Namibian women like a game of telephone – the information warping and growing more fantastical as it travels. You must boil the ink off of newspapers and then drink the concoction, still boiling hot, with hard liquor, some say. No, others advise, you must add petrol too, or it won’t do anything. Or fabric softener. Or Oros drink mix. And boil this all together with Devil’s Claw (Harpagophytum procumbens) – a root known locally to cause miscarriages.
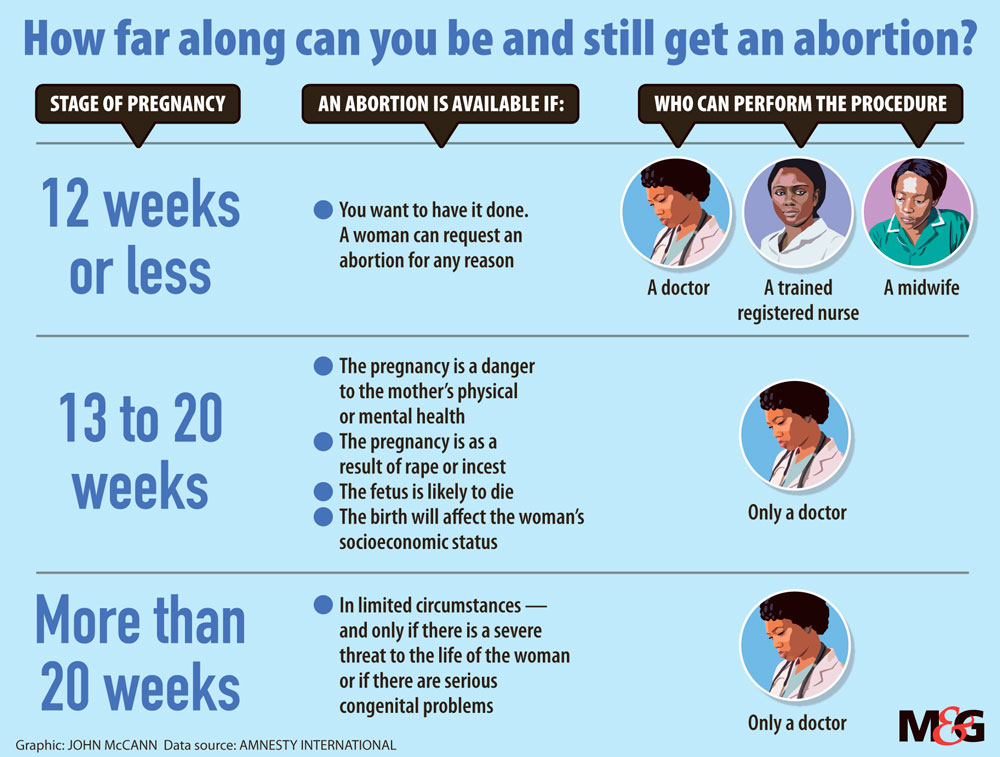
Here abortion is allowed only to save the life or health of pregnant women and in cases of rape or incest – a legal hangover from the country’s days as the South African colony of South West Africa. In the race-based, deeply Calvinistic South Africa under National Party rule, abortion was a highly politicised issue, influenced strongly by religious beliefs. A 1975 Act allowed for abortion in South Africa and Namibia in only rare instances, such as cases in which two doctors had determined the pregnancy was a result of rape or posed a threat to the mother’s physical or mental health.
When apartheid crumbled in the early 1990s, South African feminists began pushing to have the law changed and, in 1996, the country passed one of Africa’s most liberal abortion laws. But in neighbouring Namibia, where conservative Christian social norms hung low over the new liberation government, the law remained – now policing the bodies of a very different group of women.
“This is an old, imposed law that has nothing to do with our experience or our culture,” says Rosa Namises, a long-time Namibian gender activist and former MP.
Today, statistics on unsafe abortion in Namibia are, at best, blurry. A 2014 report by the health ministry suggests that up to 12% of maternal deaths are caused by abortions, but the study sample of 57 women was small.
And in March this year Health Minister Bernard Haufiku reportedly announced that more than 7 000 illegal abortions were recorded at state facilities in 2016, saying it could be as high as 10 000 because many cases go unreported. But other experts have pointed out that this number rather refers to “spontaneous abortions”, which include all miscarriages – most of which would have occurred naturally.
Nonetheless, Haufiku was quoted in The Namibian newspaper as saying: “We need to ask ourselves whether it is not time to relook the legislation and decriminalise abortion.”
His suggestion was met with vehement opposition in Parliament and Benjamin Khumalo, president of the pharmaceutical society of Nambia, says it’s unlikely that abortion will be legalised soon.
“We have a terrible situation here with babies being dumped. We see the effects of illegal abortions in our hospitals, where young women come in bleeding, with ruptured uteruses,” Khumalo says.
For those with the means and time, travelling to private clinics in South Africa is an option. But for most Namibian women, the sole choices are poisons or pills.
In Namibia, pills are probably a better option than other choices for self-terminating a pregnancy, “but it’s a mafia game”, says Tameca Gaoses, a Namibian feminist activist. On the black market, women often don’t know whether they’re getting pills that are real or fake, she warns. So, at most, the pills are the best of a collection of bad choices.
And there is little to stop unscrupulous providers from playing with the health of women.
“We are aware that pills are advertised on social media – Facebook, or even passed on in WhatsApp groups,” says Khumalo. “And we can’t vouch for each and every pharmacist. Even if the pills are not fake, there may be dangers in using misoprostol.”
Several internet providers of abortion pills in Namibia contacted by Bhekisisa claim pill-based abortions could be performed at home up to 24 weeks of pregnancy.
One provider is a single mother of four in rural Namibia who has been out of work for years. She has finished high school, she says, but the only training she has in how misoprostol worked came from her supplier in South Africa, whom she has never met. He routes customers to her through a Facebook page, which promised “WE USE SAFE & TRUSTED PILL, WE TAKE CARE OF YOU, IT’S SAME DAY SERVICE!!”
The Namibian provider says she makes about R1?000 a month re-selling misoprostol, and that she has never heard of women having serious complications from using them. She explains: “In Namibia you can’t easily find these pills. The reason we’re doing this is to help people.”
Tlaleng Mofokeng, a doctor, legal abortion provider and reproductive rights activist in Johannesburg, says there has been “essentially no crackdown on illegal pills. But when women are desperate, they will always make a plan, regardless of whether money or the law are on their side,” she warns.
Representatives of both the South African and Namibian police confirm that they have not undertaken any major investigations into the market.

Women on Waves gained international fame – or notoriety – with its “abortion boats”. Since 1999 the Dutch charity has been sailing to the coasts of countries with strict abortion laws, such as Mexico, where women in early pregnancy can board the vessel. Once they are in international waters, the women are given mifespristone and misoprostol.
Out of this venture grew Women on Web: perhaps less headline-grabbing, but with far more impact through its online portal. The organisation’s approach is “thoroughly medical”, according to the 2011 study in BMJ Sexual & Reproductive Health.
“Women are taken through an online medical questionnaire and the results are checked by a doctor,” the study explains. If no medical contraindications are found, the woman is sent mifepristone, misoprostol and a pregnancy test kit to her home address. They are counselled by phone and emailed on how, exactly, to perform the procedure, says Women on Web’s Leticia Zenevich. Should anything go wrong, the organisation has health professionals on call.
All of this is for a donation of about €70 (it is free if you cannot afford it, subsidised by other paying customers or donors).
The website states that the pills will only be sent to women who are not yet 10 weeks pregnant and who live in countries where there is no legal avenue to terminate pregnancies. They have never had a woman lie to them about how far along she is in her pregnancy, claims Zenevich. “We trust women,” she says.
And if Women on Web do not dispatch the pills, there is information on other avenues to explore: a world map gives country-by-country information on abortion laws and possible abortion providers, where ?misoprostol is available and under what brand name.
In Namibia, explains Khumalo, no pharmacist may dispense misoprostol without a prescription from a doctor – and the prescription has to indicate what it is intended for. “It has to be kept under lock and key and only the pharmacist can keep the key,” he says.
Women on Web’s advice for its section on Namibia is to order abortion pills from its website because Cytotec is so difficult to obtain in the country.
[WATCH] How to spot an illegal abortion
At Disa Sexual and Reproductive Health Clinic in Johannesburg, where Tlaleng Mofokeng works, doctors do not perform medical abortions on patients who they cannot follow up with in person shortly after the procedure, in case aftercare is required.
“Women should be asked as much as possible about their medical history so that we understand exactly the stuff that’s going to predispose them to complications. But should complications happen, they also need to know where to go – if they’re bleeding too much, if they’ve got cramping, if they’ve got pain,” she says.
Women on Web advises anyone who thinks she might have a complication to go to a doctor immediately. In places where abortion is criminal, they can tell medical staff they had a spontaneous miscarriage, the website suggests.
Misoprostol taken under the tongue, as recommended, should dissolve within 30 minutes but traces of pills may be found in the vagina for up to four days after inserting them. If the pills were taken vaginally, women should check with their fingers to make sure they are dissolved, the website advises.
But these risks to already vulnerable women – who are often scared and with no one to confide in – concerns Sindisiwe van Zyl, a South African doctor and patient rights activist whose campaign to provide medical advice on social media has garnered her a huge following on Twitter.
“We are talking about countries where you can be arrested for being an abortion provider,” she explains. “My concern is also about the aftercare, about counselling.”
Women with little access to information will find it hard to distinguish scrupulous organisations ?in the online minefield of misinformation and false claims, Van Zyl warns.
“If you order pills on the internet, you don’t know if they have been approved or where they are from,” she warns.
Among the women who seek out advice from the Amsterdam-based Women on Web every year are hundreds from Southern Africa, according to data provided by the organisation. Last year, though, only 63 women in Namibia asked for their help – a fact Zenevich attributes in part to poor access to the internet in the country.
But although these women may have had a safe option, Mofokeng says, it is important to look at the bigger picture. And that picture is not to say: “Okay, we’ve won.”
“We need to move beyond these quick and desperate measures. We also need to make sure laws reform to make abortion legal where it’s illegal,” she says.
For women like Alice, it’s hard to imagine that the rising availability of misoprostol has been particularly empowering.
“We do this because it’s the only choice we have. We know it’s very dangerous,” Alice says. “The only thing that can make it better is if government does something” to legalise abortion.
Alice now works in a clothing shop in downtown Windhoek and is saving to go back to school to become a teacher.
“I want to go back to my village and teach girls all the things that I didn’t know,” she says. “Back there, girls don’t have any access to information about what they can do if they fall pregnant. It’s small, but maybe at least I can change that.”
This story was supported by a grant from the Taco Kuiper Investigative Journalism Fund, run by Wits Journalism.

Ryan Lenora Brown is a freelance reporter, editor, and researcher based in Johannesburg, South Africa.




Adri Kotze is a senior investigative journalist and Bhekisisa's former Africa editor. Follow her on Twitter @adrikotze.




{kind=link}