

- People are more likely to follow COVID-19 prevention guidelines (such as mask-wearing and hand washing) when governments explain why the rules are put in place.
- Regulations that promote responsible drinking will be crucial as South Africa prepares for the third and fourth waves of SARS-CoV-2 infections.
- South Africa needs more skilled experts that can decode the genetic sequence of SARS-CoV-2 samples. This will help us to identify new variants quickly and better inform policy decisions.
We’re past the worst of our second COVID wave, but experts warn that South Africa will almost certainly be facing a third and fourth wave — possibly with more infections and deaths than in previous waves.
A third wave could be only three months away, amidst a new, more infectious SARS-CoV-2 variant (the virus that causes COVID-19), 501Y.V2, that emerged during our second wave and is now dominant in South Africa. The new variant has also changed itself in such a way that it can evade the antibodies that our bodies produce in response to the original version of the virus.
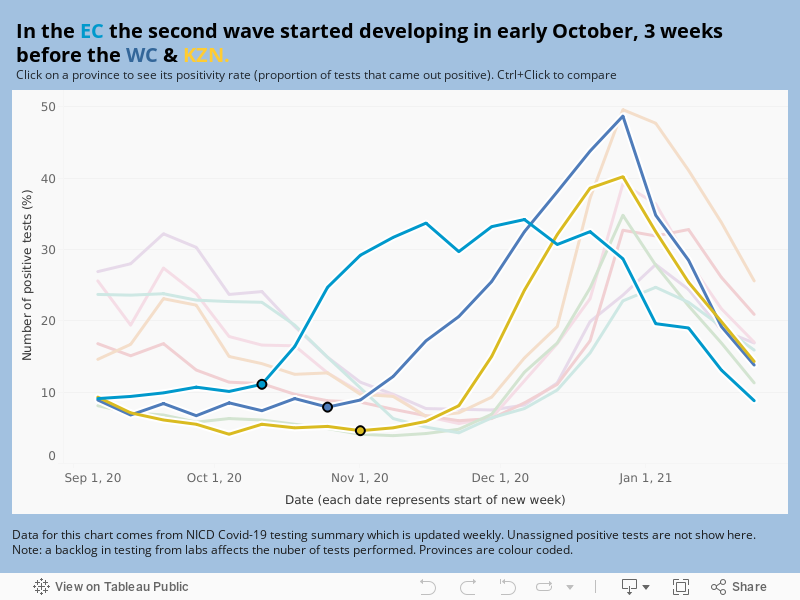
We’ve created an interactive map to show you how SARS-CoV-2 spread through South Africa between September 2020 and January 2021 (during this time the new variant, 501Y.V2, became dominant).
Last week, South Africa started to roll-out Johnson & Johnson vaccines that are 85% effective in protecting against severe COVID disease (the type of COVID that makes people end up in hospital or die) in the country.
By the time that a third wave hits South Africa, only a small proportion of the country’s population would have been immunised — not close to the two thirds the government says is needed for herd immunity (herd immunity is when a large portion of a community [the herd] becomes immune to a disease, making the spread of disease from person to person unlikely).
More new variants could emerge within the next few months, scientists say. This could have an effect on how severe our next wave will be and how many vaccines will work in South Africa.
We look at lessons South Africa can learn from the second wave to be better equipped to survive the country’s next surge in SARS-CoV-2 infections.
1. We need to do more genomic sequencing — so we can identify new variants quickly
South African scientists notified the World Health Organisation about the identification of 501Y.V2 in the country on 18 December. They were able to detect the new variant early in the second wave because South Africa has an established network of labs that specialise in something called genomic sequencing. Genomic sequencing allows researchers to decode the genes of viruses and monitor how they change over time.
A genomics team led by the KwaZulu-Natal Research Innovation and Sequencing Platform (Krisp) at the University of KwaZulu-Natal, detected 501Y.V2 during routine sequencing of SARS-CoV-2 samples. South Africa has sequenced about 3 500 genomes (virus samples) in total — “about 300 per month” since March last year, when the country recorded its first COVID case, according to Richard Lessells. Lessells was one of the Krisp scientists who co-discovered the 501Y.V2 variant.
Compared to other African countries, this number is high. Lessells says, South Africa does about half the continent’s sequencing. We also help other African countries, such as Mozambique, to sequence their viruses.
But compared to a country like the United Kingdom (UK), South Africa’s capacity to decode viruses is low. The UK has sequenced more than 280 000 genomes since the beginning of their outbreak, according to the COVID-19 Genomics UK Consortium.
The more sequencing scientists do, the more data is available to answer questions we all have about the virus. Such information also helps us to develop better programmes and policies to contain the virus, Lessells says.
Information we get from unravelling SARS-CoV-2’s genetic codes has, for instance, helped policy makers understand that variants could affect the efficacy of vaccines. In the case of the AstraZeneca jab that South Africa purchased in January, sequencing data helped researchers establish why the jab provides low protection against mild to moderate COVID in South Africa, but much higher protection in many other countries. When scientists took a closer look at the SARS-CoV-2 viruses of the South African study participants who developed COVID, they learned that about 90% had contracted the new variant. The government used that information to adjust our roll-out policy: instead of starting off with AstraZeneca vaccines, we’re now using Johnson & Johnson jabs, which provide better protection against 501Y.V2.
But how do we expand our sequencing capacity — what is it that we need more of?
We’ve got enough sequencing machines and lab technicians to feed virus samples into computers, Lessells says. “What we’re lacking is people who can process and analyse the data the sequencing machines produce.”
For this, Lessells says, we need more bioinformaticians. Bioinformatics is a specialised field of biology that is concerned with how information moves within biological systems or living things. Lessells explains that people like the director of Krisp, Tulio de Oliveira, use “computer programmes and software … to do that data analysis” and bring us closer to answering questions we have about the virus.
De Oliveira is the bioinformatician who headed up the team that discovered 501Y.V2.
To qualify as a bioinformatician, it can take between six years to get to masters level and up to nine years for a PhD (which are the qualifications needed to get hired), according to Eduan Wilkinson, a bioinformatician at KRISP. South African universities that offer biomedical science qualifications include the Rhodes University, University of the Western Cape, Stellenbosch University, University of the Witwatersrand, University of Pretoria, University of Cape Town, University of the Free State, Nelson Mandela University, University of KwaZulu-Natal, University of Limpopo, University of Venda mostly as a postgraduate specialisation.
The department of higher education, science and innovation, has allocated R25- million to Krisp to sequence a further 10 000 genomes, or virus samples, from both South Africa and the rest of the continent over the next 12 months.
2. Complacency is dangerous: Target it
Public health experts got concerned about complacency towards non-pharmaceutical measures such as mask-wearing, hand-washing and social distancing during the second wave — also now that the peak is over.
Videos showing how even government leaders don’t adhere to these measures are frequently circulated on social media — from people gathering in large crowds without masks, to individuals spreading misinformation about the value of masks, to rave parties without any sign of masks or physically distancing.
Political parties such as the Economic Freedom Fighters have held protests without adhering to social distancing and government officials like Mpumalanga’s Premier, Refilwe Mtshweni-Tsipane, have attended funerals without wearing masks.
Non-compliance has also been acknowledged by the health department. Health Minister Zweli Mkhize has, for instance, recorded video messages about the need for compliance that he distributed on Twitter. He has also conducted late night visits to nightclubs to monitor if patrons play by the rules.
Masks help to prevent the transmission of SARS-CoV-2 by stopping the spread of respiratory droplets when people talk, sneeze or cough. Since we still don’t know how well vaccines prevent us from spreading the virus (we only know that the jabs protect us against falling ill with COVID), we will need to continue to wear masks for the foreseeable future, even after vaccination. Learning how to get better at wearing them, would therefore help us to be better equipped for the third wave.
Atiya Mosam, a public health medicine specialist from the South African Medical Research Council’s Centre for Health Economics and Decision Science, admits not all negligence is wilful. “When our routines normalise it becomes easy to forget that we are in a pandemic,” she says. “It’s easy to forget to put a mask on, on your way to the kitchen in the office.”
But there are strategies that we can use to increase compliance — and lessons to learn from other countries.
Mosam says we need to “make the environments surrounding people amenable to them following… regulations”. In some respects, South Africa is already doing that — for instance, by having manned sanitiser stations at the entrances of shops.
The WHO has studied ways for countries to tackle non-compliance.
The organisation says evidence shows that compliance messages are less effective when they are packaged as “do not” messages as opposed to “do differently” notes. “Appeal to people rather than blame, scare or threaten them,” the WHO says. “Avoid judgement and blame related to risky behaviours, as this can contribute to shame and alienation more than engagement and motivation.”
Also, when governments and scientists are consistently transparent with explaining the reasons for such measures, and also prepared to acknowledge the limitations of science, the trust in such tools increases and leads to better compliance because more people perceive them as fair and necessary restrictions on their freedom.
In some countries, leaders have sought to lead by example. For instance, “when quarantine was deemed necessary in Germany, Chancellor Angela Merkel self-isolated from 22 March to 2 April after her doctor tested positive for the virus”, the WHO explains. Afterwards, she recorded a podcast about her quarantine experience and shared that she had been lonely.
In South Africa, Mkhize also announced that he and his wife would quarantine after they tested positive for COVID in October.
Buy-in to adhere to public health measures is also higher when the public is allowed to help shape such measures. The Danish Lung Association, for example, created a campaign for young people, “encouraging them to enter a competition to come up with ideas for how to spend time together in a safe way during the pandemic”, the WHO reports. They explain: “Actively involving target groups in the design and delivery of engagement activities can ensure that they are tailored and responsive to the perspectives and experiences of the people they strive to reach.”
And in Turkey, the WHO country office conducted Twitter polls asking questions such as “What are you doing to protect your health?” “These types of low-cost engagement activities,” the WHO says, “may spur people to think critically about their own behaviours and social environments while serving as a reminder of the ongoing pandemic.”
3. Slash the number of binge-drinkers at home and on the roads
During both the first and second COVID wave, the government implemented either a total ban on alcohol sales or restrictions on the days and hours during which alcoholic beverages could be bought.
Almost 200 people die of alcohol-related illnesses and accidents in South Africa each day, a 2018 BMC Medicine study has found. Our problem is binge-drinking — when you drink 5.4 standard drinks in one sitting — that research has shown frequently leads to violent incidents. Although a little less than a third of adult South Africans drink alcohol, almost six out of 10 drinkers engage in binge drinking, the WHO reported in 2018.
Restrictions on alcohol sales were implemented to reduce alcohol-related trauma cases to open up more hospital beds for COVID patients.
[WATCH] Why South Africa banned alcohol under the COVID-19 lockdown
And it has worked. In the Western Cape, the level three lockdown alcohol sales ban slashed alcohol related trauma admissions by 40 to 50%, according to Western Cape health department data. When the alcohol sales ban was lifted in July, daily admissions to trauma centres in Western Cape hospitals shot up by 62%. And in the Eastern Cape, deaths from trauma incidents increased by more than 300% in the month after the alcohol sales ban was temporarily lifted.
Now, experts say, South Africa needs to adjust the alcohol sale restrictions we used during the first and second wave to become more sustainable so that they can help to reduce harmful alcohol use in the long-term.
The director of the Southern African Alcohol Policy Alliance (Saapa), Maurice Smithers, says we need to do four things.
The first is to put restrictions on the sale of beer in large containers, such as 750ml and one litre bottles. People who drink from an above average size container are about eight times more likely to drink heavily than those who drink from regular vessels, 2018 research published in the journal Substance Abuse Treatment, Prevention and Policy, found. And a 2018 WHO report shows that beer is the most commonly consumed alcohol product in South Africa.
Smithers says that unlike wine and spirits, “once you open the bottle [of beer or cider] … you can’t cork it and put it back in the fridge”. This creates a situation “where people feel the need to finish every beer or cider that they open”.
Secondly, South Africa can do a better job of controlling who has access to alcohol. “We need to increase the legal drinking age from 18 to 21 years,” says Smithers. This is already being considered under the 2016 Liquor Amendment Bill, but last year the president sent it back to parliament amid doubts about its constitutionality.
Other experts, such as the South African Medical Research Council’s Charles Parry, argue that the banning of alcohol advertising, except in liquor shops and on online sites that sell alcohol — regulations proposed by the 2013 Control of Marketing of Alcohol Beverages Bill — would also help.
A review of 13 studies published in the journal Alcohol and Alcoholism in 2009 found exposure to alcohol marketing increased the likelihood that young people would start drinking. In adolescents who already drank, seeing adverts for alcohol products increased the amount they consumed.
The 2013 Bill has, however, never been made public. Moreover, Smithers says, the price of alcohol needs to be increased. During his budget speech on 24 February, Finance Minister Tito Mboweni announced an 8% increase in the tax that alcohol manufacturers must pay to the government. This percentage is higher than the usual annual hike and amounts to nearly 4% increase above inflation.
Saapa applauded the minister’s choice to publicly explain that the government is increasing excise tax in a bid to slash harmful alcohol use in South Africa. How is that possible? Increases in excise tax go hand-in-hand with increases in the price that consumers have to pay for alcohol, which makes it less affordable, Smithers explains.
This kind of tax should be considered to be a health tax, which “finance ministers should not have to apologise for increasing… if it [goes toward] making South Africa a healthier & alcohol-safe country”.
[Update 25 February 2021 04:30 This story was updated to reflect details of Finance Minister Tito Mboweni’s budget speech on 24 February].

Mohale Moloi worked at Bhekisisa as a television producer and health journalist from July 2021 to March 2024.



{kind=link}